
We had an ill child in our A&E for over 20 hours yesterday. Read that again – yes its true – 20 hours in an inner-city A&E – on a Friday. Actually she isn’t a child – according to half the professionals that saw her, but was according to the other half. Conveniently for each of them they were able to define her in a way (wrong side of of her seventeenth birthday) that meant neither had to take responsibility for her. A definitive safe place of care was eventually found at an adolescent mental health facility over 100 miles away. Throughout this whole episode she was suffering an acute psychiatric illness.
Fragile Minds
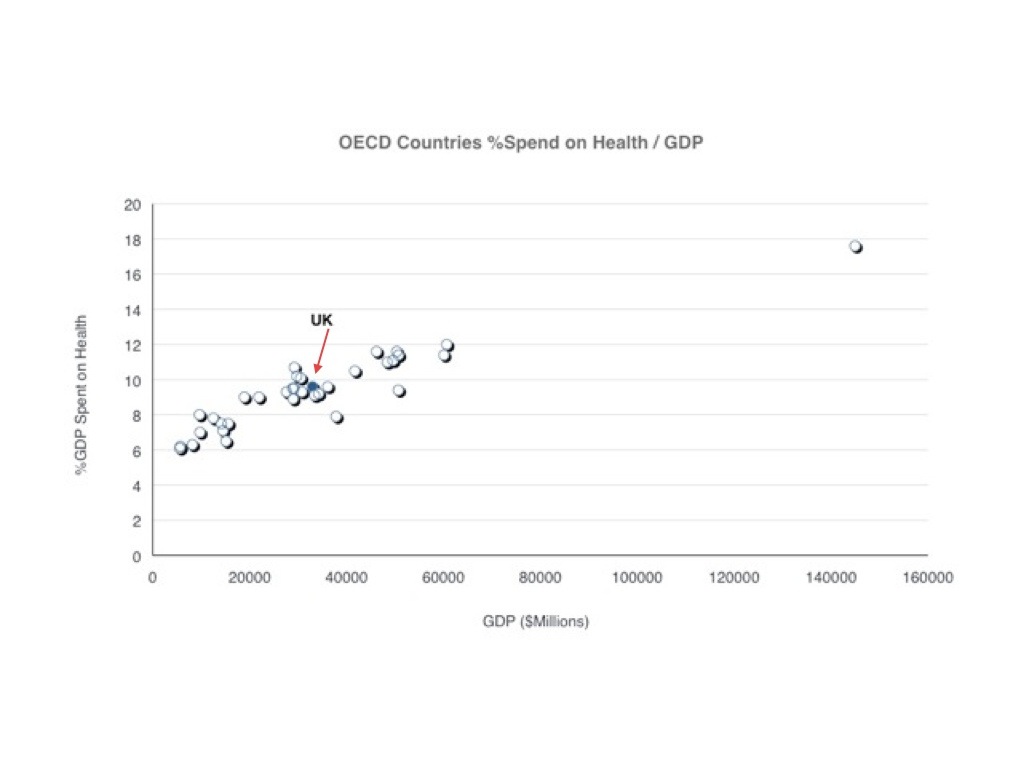
After toddlerhood – adolescence is the most active phase of brain development. It is a critical period during which personality, skills and traits are developed that set the patterns of mind, thought and behaviour for the remainder of adult life. It is a crucial phase of transition from childhood to adulthood – a period of ‘finding ones place in the world’ apart from the security of parents and family. It is an intensely psychologically vulnerable time – one of which we all have memories of our own we would probably rather forget. It is also the commonest period of life for mental health issues to first develop – by some estimates up to 20% of adolescents and young adults are experiencing some degree of mental illness and over 40% of adult mental illness commences in the adolescent period. The combined assaults of alcohol, drugs, sex hormones and dramatic changes in life circumstances on a fast developing brain have unpredictable consequences – which for a growing minority include breakdown, psychosis and the roots of devastating life long mental illness.
When your world falls apart
Psychosis is the most terrifying symptom of disease. It is the awakening of primal fears – normally locked away by evolution and civilisation. Psychosis is the manifestation of every self doubt and vulnerability we harbour, a total loss of security. The very ground you stand on loses its solidity, the certainties of perceived reality evaporate. Paranoia is intense, everyone is against you, every sound becomes the whispering taunting voices – undermining and aggravating self doubt.
During this potentially lethal psychological experience – our service finds it most appropriate to leave the sufferers sitting in A&E cubicles, overseen by security guards and witnessed by the drunken fray that make up the core clientele of A&E on a friday night. Meanwhile professionals play ‘pass the buck’ – skulking guiltily in the background too nervous to engage with a ‘difficult teenager’ – the behaviour surely being noticed and fuelling the paranoid beliefs of the patient ‘for whom no-one cares’.
Why do we do this? Why do we let down such a vulnerable group in such a catastrophic manner?
Too Special to Touch
Throughout my career I have witnessed, and been exasperated by, the phenomenon of medical super-specialisation. This is the process by which small groups of sub-specialists – usually based in well resourced centrally located university hospitals – develop standards of care for a sub-set of a population with a branch of a disease that produce significantly superior outcomes for those patients. This isn’t a problem in itself – this is how the frontiers of medicine move forwards. The problem arises when this standard of care – attainable in the rarefied environment of the academic centre – becomes the expected standard in all healthcare settings. A process of centralisation of care then ensues – as ‘good enough’ becomes the victim of ‘perfection’ – standard care in general settings is discredited. Generalists are stripped of the right to provide certain aspects of care – patients are diverted to diminishing numbers of ever distant specialist centres – as the skills for providing even ‘good enough’ care at local centres evaporate.
One of the most striking areas of medicine where this has happened is children’s services. Most paediatric services are now provided by centrally located children’s hospitals – these highly specialist tertiary centres do a fantastic job – but to survive they have had to grow their business ‘down the value chain’ to the point where they now also provide the bulk of standard secondary care. This has resulted in the shrinking of paediatric services in district general hospitals to below critical mass levels – many paediatric services have closed – many others are teetering on the edge of viability, even in quite large general hospitals. It is reaching a point where in many hospitals it is just unsafe to be a child – and the doors are simply closing on them.
This march of progress wouldn’t be a problem if wasn’t for the fact that very sick children – whether physical or, as in our story above, mental – still come to A&E expecting life saving treatment. Our doctors, with dis-credited general skills, diminished exposure and experience – are not only discouraged but actively criticised for trying to provide good enough care. So they have stopped – and patients languish in A&E awaiting transfer to over subscribed specialist centres – not receiving immediate care they need that might prevent harder to treat long term conditions. Meanwhile the generalist tiptoes around them – too terrified to touch.
A Relentless Epidemic
Childhood and adolescent mental health is very special indeed. Most ordinary doctors are scared of mental illness – this is hived off very early in training – and even more scared of children. Yet the story of our seventeen year old in crisis is becoming more not less common, what was a handful a year presenting to our A&E has become dozens a month. We don’t know why – but the wide availability of cheap alcohol, potent cannabis, met-amphetamines, and other ‘legal’ highs along with the as yet un-evaluated impact of the psycho-social complexity of a life lived ‘on-line’ must all be playing a part. And this is a drama that is being played out in emergency departments across the NHS – daily.
There is an urgent need to find a solution for delivering safe ‘good enough’ care for these patients – at the point of presentation – until a place of definitive care can be found. The needs are not complex – but they do transcend organisational boundaries – the ability to provide safe dependable holding treatment in an urgent mental health situation – is a good test of health system integration. The care of the intoxicated, potentially physical injured patient that is in the throes of a mental health crisis requires professionals that normally work in isolation (traditionally somewhat distrustful of each other) to come together and meet the physical and psychological needs of these patients.
Above all this needs system leaders to come together, organise their services to deliver and demonstrate that – yes, we do care about this calamity – we care very much.











A thought provoking piece that provides a more optimistic view of human intelligence compared to AI. Just as an athlete…
[…] https://rogerstedman.com/wp/blameworthy-acts-in-a-blame-free-safety-culture/ […]
[…] that most people would agree we need to promote, foster and support in healthcare. This piece; Blameworthy acts in…
Great blog. Your matrix, which shows psychological safety as being a pre-requisite for learning, aligns with Deming's (usually overlooked) principle…
Great post Roger. Spot on. Having now stopped clinical practise but still deal with clinicians on a daily basis, I…